Video Library
Bobby Jones CSF Ask the Expert with Dr. Jeffrey P. Greenfield
VIRTUAL MEETING - MAY 21, 2020
COVID-19 won't stop our educational efforts! Despite the global pandemic, the medical professionals on our medical advisory board have generously agreed to continue our programs remotely.
Dr. Jeffrey Greenfield of
Weill Cornell Medical Center was the first, brave expert to educate patients and family members impacted by
Chiari,
syringomyelia and related disorders virtually.
Based on a previous educational meeting in New York City, Dr. Greenfield answered questions that were submitted by real patients affected by Chiari malformation, syringomyelia and related disorders... some questions were asked in real-time!
This video is jam-packed with information ranging from the impact of the
novel coronavirus on Chiari patients, recovery from decompression surgery, tethered cord syndrome, idiopathic intracranial hypertension (pseudotumor cerebri), CSF leaks, scoliosis and syrinx, and so much more!
Interestingly, a lot of the answers to these questions were all based on relatively recent research, a lot of which is being done by Dr. Greenfield the many physicians on our medical board. Watch the full video to learn more about Chiari malformation, syringomyelia, and the many disorders that neurosurgeons, neurologists and neuroradiologists have to consider to correctly diagnose and treat patients who may be struggling.
This presentation was given on Thursday, May 21, 2020 and was presented entirely online. (2020)
Note from Bobby Jones CSF: We want to take a moment to sincerely thank all those who donated in support of this virtual presentation. No one at the organization was expecting that much generosity during such a difficult time for us all. From the bottom of the hearts of our boards, staff and volunteers, we want to thank you for your donations. Your kindness continues to motivate us and makes us all the more certain that this work is valuable and helping the people who need it. Thank you.
Video transcript:
[Kaitlyn] Okay.
Hi, welcome everyone.
I'm really glad you could all join us for our first virtual educational programming. We have Dr. Jeffrey Greenfield here today. I'm just going to quickly introduce him Dr. Greenfield is a board-certified neurosurgeon specializing in pediatric neurosurgery, but he also sees adults. He is at Weill Cornell Brain and Spine Center. He is the creator and director of the ChiariCARE program, which I believe we're going to talk about a little bit today. He is internationally renowned for his work with patients who are suffering from Chiari, syringomyelia, tethered cord, a lot of the different issues that we're going to really talk about today.
So, with that I'm going to just briefly send it over to Dr. Greenfield to introduce himself if he would like and we can get started.
[Dr. Greenfield] Are you going to introduce yourself?
[Kaitlyn] Oh!
Okay, well-- Hi, I'm Kaitlyn Esposito [laughs]
I work for the Bobby Jones Chiari & Syringomyelia Foundation. I'm pretty involved in a lot of the research programming that we're getting underway, which I hope we can talk a little bit about Dr. Greenfield's been on those calls so, we can talk a little bit about that, but if anyone ever has any questions, you can find my email address on the website. I don't know if Mary or Dorothy want to introduce themselves or if anyone else is online. We can started—
[Dr. Greenfield] For those of you who have found this through Bobby Jones CSF, you already know about their organization and their recent rebranding, renaming, but I really encourage all of you to spend some time going through the website. It's been beautifully redesigned and literally has hours and hours of videos from amazing surgeons, neurologists, internal medicine doctors, pain management doctors-- I mean, it's an amazing resource for people who are looking for information, who are looking for people that are in their part of the country.
Clearly, video has let us all connect in a way that we didn't think possible just a short while ago, but it's also really nice to be able to see people near you, so we'll talk a little bit about what that all means for the future of neurosurgery, hopefully at some point tonight.
I do want to thank Kaitlyn, Mary, and Dorothy-- I mean, their organization has single-handedly brought a number of important initiatives and clear direction to the world of Chiari that didn't exist ten years ago.
And Kaitlyn was alluding to a new initiative, led by some of the board members at the CSF organization that are truly looking at a new way of analyzing patients so that we can better predict who is going to be a good candidate for surgery, how do we advocate for patients, which type of surgery should a patient have, how do we follow them?
And creating some standardization so that-- so much of the frustration that we hear from patients might be minimized in terms of variability in what you're hearing for evaluation surgical goals, who's a good candidate what kind of surgery to do-- and so, hopefully we can create some standardization in a way that many other fields have done in neurosurgery.
Chiari has always been a little bit of a hard field to characterize because it falls into so many areas: pediatrics, pain management, CSF disorders, spinal disorders... So no one's really ever taken the whole-- but now that there are a number of people around the country who have really made it their focus, and their initiative to come together, I think you're going to see a
tremendous amount of research and data coming out.
I'm going to highlight some of that today-- some of it I'll talk about is my own, but hopefully, data that's coming out from a lot of the consortia and collaborations that are years old and will bear fruit for years to come. So, thanks to the CSF. You really can't say enough great things about the organization.
With respect to tonight, I think that Kaitlyn and I just brainstormed that this might be a nice way to connect people during a really trying time in everyone's lives. We're all adapting to a new mode of medicine and um— I've been seeing patients remotely and I can talk a little bit about what coronavirus and COVID has been like in New York City at the epicenter, if anyone's interested or curious.
But I think that this was something that we just said let's just see if there's interest in it and we can certainly never answer everybody's questions in 60 minutes, and so you know- what I think Kaitlyn and then Mary will do later is hopefully follow up with everyone and see if there's some consensus in what topics they'd like to get covered or didn't get covered and we can have specific future sessions to— more narrow aims and then hopefully I can convince some of my partners in crime around the country, other folks on the board who you guys know so well to contribute as well and do some similar seminars.
The diversity of voices is what makes this organization strong-- it's certainly not any single person. With that, I'm gonna let Kaitlyn run this a little bit, and maybe offer up some questions to me. I've seen all of the questions that have been submitted. I may take the liberty of kind of combining some of them, and overlapping them-- trying to get as many people's questions if I can. If I don't get to your question, I apologize. It may be because it's really complicated and difficult and it may not fit in this form. It may be because it's too personal and it might be better just for us to have a conversation and Kaitlyn or Mary can get you my email, or figure out how to get in contact with me. Some of you wrote in some pretty specific questions that probably should just be addressed between doctor and patient, so— with that, thank you very much
for coming and thank you, Kaitlyn, and I guess we can get going!
[Kaitlyn] Okay. I will add to that-- that we absolutely do plan on doing this again, so if your question is not answered and it's not that it was too personal and better handled person-to-person, we will do this again. So, definitely stay tuned for that.
I think I'm gonna start with kind of how you introduced everything— with— as far as how COVID is affecting Chiari patients. Because I know we've gotten a lot of questions from concerned family members, parents— is there any way that Chiari patients are more susceptible to this pandemic? Or, are at more risk? Is there any way you can speak to that?
[Dr. Greenfield] It's a tricky question, but I think it's worth talking about. I mean, everybody here both has a connection to Chiari and has been affected by COVID. So, I think it's probably worth talking about.
So, NYC essentially shut down on March 15th, and all surgical-- you know-- and outpatient activities essentially stopped on a dime. It was really unprecedented in terms of the response that we prepared for and generated. I can't speak highly enough about how all the hospitals in NYC and now, unfortunately, in other areas around the country have been responding to it. It's really been dramatic. I felt a little a little bit left out, to be honest. My skillset as a neurosurgeon was particularly useless in terms of taking care of patients with respiratory problems, and lung issues, and ventilators.
So, we've been taking care of a lot of research and catching up on a ton of writing up papers and collaborating with people. So, it's been wonderful for us but-- I've missed taking care of patients, for sure.
We've started doing video visits in the absence of face-to-face time I think that this has bit of a revelation for us in terms of how well it's worked. So much of what I do in my consultations with my patients, as you know, is talk. You know, it is nice to have a neurologic exam and it's nice to be face-to-face, but sometimes it's just catching up-- it's discussing symptoms and for patients who are around the country, patients who feel vulnerable about traveling at this time, people who have difficulty traveling, who have difficulty coming to NYC or other major cities where a lot of the Chiari physicians happen to be located, this can provide a really nice conduit to get some information, create contact and then decide on follow up.
In terms of how it's impacted Chiari patients, I think it may be in ways that we haven't necessarily-- not have anticipated. As we've been coming back online and we've been slowly ramping up operations again, in a literal and figurative sense, Chiari patients have gotten a little bit left behind because they often get viewed as elective, chronic patients, and we've been focusing on high acuity patients. It's a hard battle to fight at the administrative levels. You know, patients who have ruptured aneurysms or brain tumors or spinal cord compression are now getting operated on fairly regularly and trying to triage a limited number of operating rooms and resources and PPE has been the trick.
And so, we're slowly coming online and we're doing the best we can. But I think-- I didn't anticipate the effect would necessarily be that we'd be putting off so many surgeries and seeing patients because of this. It's largely because of how the medical community views Chiari in a sense. In terms of specifics on how this may affect patients who have Chiari, I think-- you know-- in terms of, some of the co-morbid conditions that affect so many of you, I think that the overlaps that I see in patients who may be susceptible: immunocompromised who might have issues with some of these overlapping things like mast cell disorder, patients who are on chronic steroids, patients who are on chronic medications for IIH, patients who have implantable devices... I think we sometimes underestimate how fragile some of you may be-- we, meaning the medical community. And I think it's both been challenging to figured out how to take care of you but also reassuring to know that we have all these options and alternatives with video consultation.
In terms of my own practice, just so you guys know—since so many of you look like familiar faces-- it's a good time to announce that we're now officially collaborating with Columbia University. So, Cornell and Columbia which are both under NY Presbyterian Hospital, it's actually now one pediatric neurosurgery service. And we're operating at children's hospital uptown, and at Cornell University downtown. The adults will probably be mostly at Cornell and a lot of the kids will be uptown, because they're opening a little bit sooner.
This is gonna essentially create a really nice, large collaborative group of highly talented partners of mine now. That'll be really nice and give a lot of options and alternatives as things roll out in NYC more slowly than in other parts of the country.
So, I'll leave it at that--I don't think I want to comment too much in terms of specific cases. There are people who have immune deficiencies and other types of issues that I think are really addressed best one-on-one with your doctors, but clearly we take these things into account when we're deciding timing of surgery and effects of travel.
[Kaitlyn] Absolutely. Yeah, and there's obviously so much we don't know about the viral infection itself. It's hard to make any kind of statement-- if we just don't know.
[overlapping discussion]
[Dr. Greenfield] In terms of-- I know there's been a lot of concern about what the hospitals are like-- and what does it mean to go into the hospital? If you have to have surgery? I'll just say that, um-- I've been completely reassured and comforted being in the hospital and in the operating rooms the last few weeks.
Particularly the children's hospital-- there is no more coronavirus, or COVID and some of the post-infectious issues that you might've heard about in the news are all in patients who had had infections weeks or months ago and are not infectious anymore. And they're all doing quite well.
So, the ORs are operating fairly normally. It feels like a normal hospital-- it's just a little bit quiet. And there's a little bit of a decreased flow-- we're trying to keep visitors to a minimum, we're trying to keep extra people [home]-- there are no medical students hanging around, no vendors hanging around. So, it's just a little bit calmer and quieter... and in that sense, it's actually been nice. But, we haven't really seen any effect in terms of quality of care, and there's certainly been no transmission between patients so if there's any concern about that, I hope I can allay those fears. If you're ready, and you need to have it anywhere in the country, as long as they're following the CDC and WHO guidelines, as most hospitals are, you should be completely safe. Just wanted to put that out there.
[Kaitlyn] To piggyback off something you said earlier about joining up with Columbia, I know there are a lot of Chiari patients that travel to see specialists. So, if someone was say, further away, or even on the other side of the country how would they be able to interact with your institution, specifically? Understanding that there might be differences site-to-site.
[Dr. Greenfield] Yeah, I have to say, Kaitlyn, this has really evolved over the past two months and I think it's been, maybe, one of the silver linings of COVID that we've been figuring out how to deal with the distance. And the lack of social interaction has been-- initially I thought it was going to be really devastating, but I think it's been really nice because it's opened up all these opportunities to create video consultations and -- start conversations that might have been more difficult to do in the past.
And so, now we can essentially say, if you're interested in seeing patients--and, again, I'll speak for myself, but I don't think this is different for anyone around the country--I know everyone on the board fairly well and if you connect with people's offices, they pretty much want some basic level of background information. They like to see at least your original scans and your most recent scans, any operative reports if you've had surgery before, and then usually some other medical notes, whether it's from the ophthalmologist, or neurologist, or urologist [cough] about issues you're having and then with that information, it's pretty easy to get a video consult organized.
Doing them now, instead of having office hours once a week, I'll do two or three video visits everyday. It's a little bit more flexible, a little bit more malleable, and I think we actually are more productive in these forums, so… hopefully this will create an opportunity for things to improve in that regard.
NYC is a difficult place to travel to, it's expensive, and now there's fears about traveling because of infectious issues and even if they're unfounded, I think it'll create a nice way to connect other patients with me, and some of you guys with doctors in your area that maybe you thought were out of reach or not accessible-- they're more accessible than you might think!
[Kaitlyn] That's very true. I've been hearing that, as well.
So I'm going to pivot and ask a question that's actually come up in the chat a couple of times and we had it earlier, if we condense all the other questions... There's some research being done as far as how Chiari, even if mild, might cause cognitive symptoms, speech issues, coordination— but it's not well researched.
Is there any way that you can speak to the potential connections and how maybe we can look into this in the future as far as treatment of those really bothersome symptoms that might be for some patients?
[Dr. Greenfield] Yeah, I can't-- I can't tell you how interesting this topic is. I think that everyone on the board is interested and it's maybe a little bit of an obtuse connection-- but the fact that Chiari patients have cognitive difficulties is, um-- 100% certain in my mind.
If anyone tells you that they're not connected, I just think that they haven't done enough research, or thought deeply enough about the question because I may have been skeptical early in my career, and the more patients I've taken care of and the more people that I've seen improve in that regard, the more convinced I've been.
One of the reasons why it's been controversial is because I think there's always been a concern that cognitive dysfunction, or "slowness", whether it's difficulties in memory, or spatial relations, or speech, may be related to the fact that Chiari patients are chronically in pain. And chronic pain patients all have some co-morbid associations with depression and anxiety. And I think that that's not untrue, I don't think that that's necessarily and untrue statement that people who have chronic pain-- like patients who have chronic diseases of any sort-- cancer, autoimmune, rheumatologic, orthopedic. Yes, chronic symptoms do create levels of anxiety and depression that we don't see in the general populations, so I don't think those two things necessarily go hand-in-hand.
But at the same time, the more research that's been done, the more obvious it has become that the cerebellum and the areas of the brainstem that the cerebellum's linked to, are connected to higher cognitive functioning areas. And there's a real link between what everyone thinks is going on and what really is going on. We have an IRB at Weill Cornell that is looking at cognitive effects of Chiari in terms of neuropsychological testing before and after surgery. We have a specific battery of 30-minute tests that we've created that is specific to the types of cognitive dysfunction that we believe are common in Chiari patients.
One of the drawbacks of this has been that insurance companies don't seem very interested in paying for it-- just, you know, to be blunt. They don't think it makes a difference and that may be true in part, in terms of making the decision for surgery, but we're never gonna move the needle forward and find out whether we're on to something here or not unless we study it. And so we need to do formal testing before and after surgeries and then, in control patients who have not had surgeries to see if there's a real effect of surgery on those cognitive functions.
If I can share my screen-- am I allowed to-- I'm in charge of it right now?
[Kaitlyn] You should be able to-- Um.. give it a shot! [Laughs]
[Dr. Greenfield] Can you see this?
[Kaitlyn] .... no Let me just make sure... Let me try one more time. Here we go.. Now try.
[Dr. Greenfield] You can see that now, I assume?
[Kaitlyn] Yes.
[Dr. Greenfield] Okay. This is actually-- I didn't plant this question at all, but this is a paper that just got published this month by two neuropsychologists in my group, Ken Perrine and one of his graduate students, Stephanie, looking at the neuroanatomic correlates of why there are neuropsychological problems in Chiari patients.
We're certainly not the first group to be interested in this question, but Dr. Perrine is a really interesting guy who's interested in the connections between the cerebellum and the cortex.
And so, here are some pictures-- you guys can-- I can share this aroundwith you after the talk-- looking at the robust connections between the cerebellum and the brainstem and higher-cognitive functioning areas: pre-frontal cortex, motor cortex, SMA, even speech areas. And so, basic neuroanatomy that's been known for 100 years, has largely been ignored by surgeons and doctors taking care of Chiari patients, saying, "No, there's no way these things could be linked." And yet, real basic neuroanatomy shows that not only are they linked, they're really important. In kids that I take care of that have brain tumors in the posterior fossa and cerebellum, we know that sometimes during surgery in this area of the brain, causes something called cerebellar mutism, which is an inability to speak. And for most of you who know anything about basic neuroanatomy, it's thought that most of the speech centers are actually on the left side of the brain.
If you're right-handed, some in the temporal lobe, parietal lobe, these areas seem like they're a mile away from the cerebellum yet when we do surgery on the cerebellum, sometimes speech is affected. And so, we know this, and we know what this anatomy is, and yet it gets ignored [in Chiari].
All I can say, is I'm very hopeful that there are a number of people and groups... at Stanford, Gerry Grant is interested in this. In Rhode Island, Dr. Klinge is interested in this. Dr. Luciano at Johns Hopkins is interested in this. And hopefully we can move the needle forward a little bit, but it needs some rigorous testing and collaborative effects to really get to the bottom of it. But I'll just say, to finish this area of discussion: please push hard for your doctors to get you the testing you need. If you feel like there's a cognitive issue, you know, don't feel like you shouldn't continue to push until you get the answers you want to get. That would be neuropsych testing at a center that's familiar with it. And I think you'll reap rewards from that because you'll get real clear data on what's going on. And often, the backend of it it cognitive remediation, where you can actually find tools and techniques to help improve. So, if you're not a surgical candidate, or you've had surgery and you haven't fully improved, there are ways to improve those aspects of how those connections work. It's a really cool question and it's really interesting field right now.
[Kaitlyn] That's great. So, again, I'm just gonna keep choosing questions that kind of—
[oh, sure]
[Is it just me? Okay.]
[Just leave that up there?]
[That's fine.]
[Kaitlyn] So, I'm gonna keep piggybacking off of these other questions. So, there was a question that came in asking what type of testing you recommend be done. I know there are a lot of co-morbidities that can cause different symptoms that either correctly or incorrectly get attributed to the Chiari that may or may not get better after surgery. So, what kind of testing do you recommend to diffuse out which symptoms are related to what, and whether or not they'll get better after surgery?
[Dr. Greenfield] I'm gonna pull up a talk here while I answer this question because I think maybe some graphics here will help...
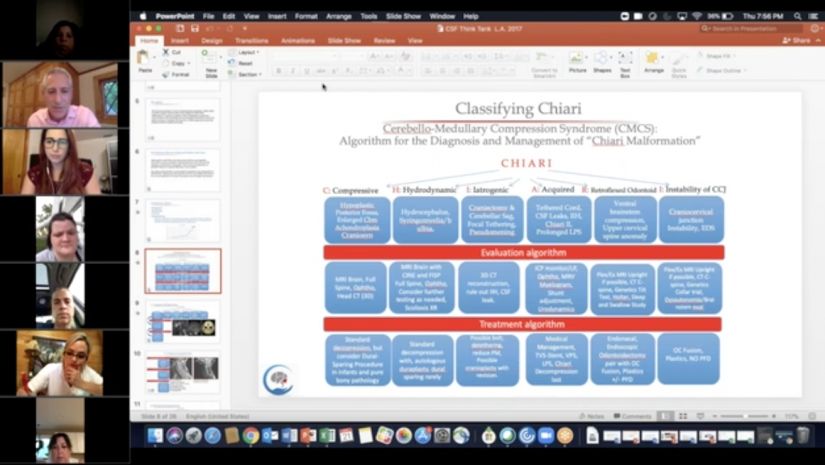
So some of you have probably seen this classification scheme before in terms of how I think about Chiari. I think that there is probably no topic that brings up more controversy when I hear from patients about what other patients have told them, or what they've heard from chat rooms about what they need to get done to be tested.
And I think-- I don't think there's a single answer here, Kaitlyn, I think that the important part of my evaluation is trying to figure out which lane the patients are in. What I mean by that is there is a very different workup that I consider to be essential for patients who have different parts of the "Chiari spectrum".
And so, again if you've seen this talk, or you've been to my office, or know how I think about Chiari, I think that Chiari is really a bunch of different diseases that all manifest with compression at the cervical-medullary junction. Right? So, the brainstem and the cerebellum are affected in one way or another. And you may be born with it. It may be acquired over time. It may be due to instability. It may be due to hydrocephalus. There are so many different ways that the same type of symptoms might manifest and so, for each of those patients, it's a little bit different in how I work them up. So, I don't want to give the illusion that there is a single list of studies that everybody needs to get.
I will say that the most common question related to this is, "Do you need to get the whole spine imaged?" And I'll say, almost without fail, the answer is yes. Not always-- but I'm going to say "not always" for everything because I think there's an art to this and I think it continually evolves. And I've changed, probably over ten years in how I've done this. So, if you have Chiari, you're diagnosed with Chiari, you definitely need to look for syrinx, you need to look for tethered cord. Those are just so highly prevalent in those populations that I always start with those. There's specific sequences that you need to do because they're often incomplete, and you need to decide if you're going to get more sequences done.
I'm just gonna plug in my computer because I see it getting low--
[Kaitlyn] No problem. Me too.
[Dr. Greenfield] And then-- so after imaging, the whole spine, then the questions are: "what else is really necessary?" For me, the only other really necessary part of the workup is almost always an ophthalmologic examination to look for signs of elevated pressure. And the reason why I've started doing that routinely on everyone is because I think that's the thing that is missed the most in adult Chiari patients. And it's the thing that creates the most complications if it's missed. It's also really easy to do and it's noninvasive.
So, the combination of being really important, helping avoid complications, and being noninvasive makes getting an opthalmologic exam something that everyone should really do routinely if they've got Chiari because it's the best way to noninvasively determine whether you have any signs of raised intracranial pressure.
And if you've got raised intracranial pressure, whether it's due to hdyrocephalus, or IIH—so "pseudotumor cerebri" is known as "idiopathic intracranial hypertension" now-- those things really need to be treated well before the Chiari even gets looked at. And so, again, my algorithm always looks at treating those things first.
With respect to some of the trickier topics, I'm gonna say that it's really on a more case-by-case basis. Because sometimes I don't need more information to make the diagnosis, but sometimes I do. And so, testing for EDS, doing dynamic imaging of the neck, getting upright imaging, doing myelograms, getting urodynamics-- you know, I can't say that I do that for every single patient because A, it would be irresponsible. It would show a lack of focus. It would be incredibly expensive. And most of it would be negative...
And so, in patients where the silo, and again, just to spend a second here since I'll probably refer to it a bunch, "compressive" is the classic Chiari, "hydrodynamic" is related to those patients who have CSF dynamics problems (like hydrocephalus), "iatrogenic" are those patients in whom something has been done to them and they've created a complication or a problem. That can be tethering, pseudomeningocele, cerebellar sag in large surgeries. "Acquired" Chiari: from leaks—which have become more and more important and I hope someone asks a question about that because it's become such an important part of my evaluations in my practice. Tethered cord, pseudotumor.. And the fun ones over here—retroflexed odontoid, and instability which are the EDS patients.
You can see the evaluation algorithm is a little bit different for each patient and even within these categories, I'll amend them or add things as necessary So, I'll just say that I think that-- if anyone tells you that there's a one-size-fits-all approach to surgery or one-size-fits-all approach to the workup, then they just haven't seen enough patients. Because the diversity of patients, the diversity of workups, is really astounding, and it's something that's made this fun, made it interesting to think about and to write about.
And so, it may be a little of a nonanswer, but get the full spine, get the optho... and I think almost everything else needs to be thought about in a really systematic way.
[Kaitlyn] Yeah, actually, too-- There have been several questions about basically, pressure issues. There are questions about-- "Is it common for CSF to leak out of your nose or your ear?"
And then, um-- if there's eye pain, or obviously, if the opthalmologic testing comes back kind of abnormal, is there a chance that those individuals would lose their sight? How do you treat something like that?
[Dr. Greenfield] Yeah, that's a nice piggyback, you're right. It just sort of flows out from this "hydrodynamic" and so maybe I can--um-- if I go to the next slide here...
[silence]
So, in the hydrodynamic pathology, these are patients who have hydrocephalus, or who have syrinxes due to hydrocephalus. I think that-- the problem has to be traced upstream. What I mean by that is-- I'll show a really cool example here that I think I posted on my Facebook page earlier this winter of a young lady who had a huge syrinx. It turns out that the patient's syrinx was from secondary Chiari. And the secondary Chiari was caused by a primary CSF leak in the spine.
And so, the wrong thing would have been to shunt the syrinx or decompress the Chiari. And I think that may have been done in many, many places around the country. For her, luckily, she complained of some really classic symptoms of CSF leaks: positional headaches that resolved when she laid down and got worse when she stood up. And so even though we don't do it very often, we did a myelogram because the CSF leak story sounded so convincing.
And, in fact, she had a leak and all we needed to do was fix the leak. It was really difficult to find, and you need really, really talented interventional radiologists who know how to do myelograms with really specific techniques. So, it's not something done everywhere. But once it was identified, the surgery to fix the leak was relatively minor, it was a small laminectomy, fix the leak. That in turn, allowed the cerebellum to ascend back into the brain, because it was no longer being pulled down, and as a result of the Chiari being restored, the syrinx went away.
So, everything was the result of one small leak in the dura in the lumbar spine, the thoracic spine-- but I could and do see the difficulty in, number one: finding it, diagnosing it. And I just know in my heart that there are so many patients out there with Chiari who have really small CSF leaks that we just can't find and it's tragic and it's hard to know what to do in those situations.
But getting decompressed in that scenario will create worsening of symptoms. We see it all the time. Kaitlyn knows that this is one of the biggest problems: failed Chiaris. It's not so much a failure of the surgery, it's a failure of the diagnosis. If you don't think about the pathophysiology from the root cause, you can get into trouble. We all do it, despite trying our darndest to find out the root cause, but sometimes we just don't see it or it's not there at the time.
Just to make the scenario even more complicated, just imagine I was right about all that-- I was so smart-- "oh, great! We figured out it's a CSF leak." And then, you don't see the leak because the leak closed by the time you did the myelogram. Sometimes that happens. And so now, you're like, "Well, there's no leak. There's definitely not a problem here. Let's do the Chiari decompression. Let's take care of the syrinx." And so, sometimes, it's not for lack of trying, but because it's a very difficult problem when you have things that come and go. Whether it's pseudotumor, whether it's CSF leaks, it creates an even bigger challenge and sometimes, despite our best efforts, it doesn't reveal itself the way we want, and the wrong thing gets done. And that's just part of this field.
[Kaitlyn] One of the follow up questions that came up in the chat is: "Is it possible to have a normal ophthalmologic exam, but it turns out that there was a leak. And if there is a leak, how long is it possible for someone to have a sustained leak without having serious issues?"
[Dr. Greenfield] Well, so... There are a bunch of really interesting things that that question raises.
Patients with really bad CSF leaks, if any of you know them or are suffering from them, then my heart goes out to you because it's really incapacitating. Patients with really bad CSF leaks really just can't live their lives. They can't stand up for more than 15 or 20 minutes. And it's truly incapacitating in so many ways.
The question about the normal eye exam is really fascinating and I suspect this is a patient who is experiencing this conundrum. Say that, unless you really see tons of patients, it may not occur to you, but you certainly can have a situation where you have no papilledema or you have no findings on the ophthalmologic exam, and you might have periods of high pressure. And these are patients in whom high pressure is actually followed by periods of low pressure.
My ophthalmologist that I work with, Dr. Dinkin, he and I very closely follow a dozen or so of these patients who have what we think is a cyclic ICP syndrome, where pressures are quite high at times, which causes enough of an erosion of the dura to create a leak. That leak then lowers the pressure, and depending on where in the cycle you happen to see the patient, or do an LP, or do a pressure monitor, or do the eye exam, you might miss it.
Papilledema sometimes is so profound that it will last long after the pressure is normal and so sometimes the ophthalmologist can detect that there is a history of papilledema, and that's really useful. But when I press all the ophthalmologists about the true number, they'll all say, "Yeah, it's not that common, but you can definitely have high ICP without papilledema." And so, I suspect those are the patients who are getting lost here.
In terms of how long you can have a leak for-- I think that was part of the follow up question, as well-- I think indefinitely. There are people who live with CSF leaks and there are people who have multiple sources of CSF leaks. And so, there are patients in whom every single nerve root has, what we call, a "diverticular", or a little weak spot. And when we see myelograms and there are weak spots all over the spine, it can be really challenging to know what to do. Because you can't, obviously, open up the entire spine and fix every single level. And so, it creates a little bit of a whack-a-mole, where to try to fix what's leaking at that time and it could be three months later, something else opens up and starts leaking once you fix one area. The truth is, it could be anywhere. And in those patients, the best thing we can do sometimes is lower the pressure with medications, sometimes with shunts. Treat them symptomatically, when possible. And if they do have a Chiari, sometimes it is necessary to do a decompression just to give them some room because they may be symptomatic, even if you know what they underlying cause is. So, it's complicated, for sure.
[Kaitlyn] So, just to, kind of tie a bow on this conversation, because it's fascinating-- CSF leaks and different pressure disorders will definitely affect-- or, may-- may affect your vision and symptoms related to that, correct? Just to make it clear.
[Dr. Greenfield] Yeah, so there are a number of ways. Just to spend a minute on the vision question, since I think that was—maybe I missed the tone of the question-- but you can get visual symptoms in so many ways.
Clearly, in pseudotumor patients, in the classic elevated pressure scenario, the problem is pressure on the optic nerves. And that's blurry vision, visual loss.
Patients with brainstem issues like craniocervical instability, a lot of EDS patients report to me that they have periods of blacking out, or floaters, or difficulty focusing. I think those are really common.
And then, in patients who have CSF leaks, sometimes we'll actually see sagging of the brain, which can pull on the cranial nerves. So, some of them can get 6th nerve palsy or 4th nerve palsy, which result in "diplopia"-- that's either difficulty conjugating your gaze up and down, and seeing double in a vertical orientation, or left and right and seeing double in a horizontal configuration.
It can really run the gamut from blurry vision, to floaters, to blackouts, to difficulty coordinating your eyes. It can really go across all those spectra.
[Kaitlyn] I'm sure there are gonna be a lot of follow up questions about this but I do want to pivot-- oh, go ahead!
[Dr. Greenfield] Opthalmologists are really key here. And neuro-opthalmology is an emerging field and, you know, I work with a group of fantastic neuro- ophthalmologists and they are really invaluable to this diagnosis and whether you've got pseudotumor or Chiari and you come to see me, you will see an ophthalmologist as part of it because I think it's so critical to diagnosis and workup. They're really important. And you can do this almost anywhere in the country as part of your workup so I highly recommend it.
[Kaitlyn] They're your friend! For sure. I feel terrible having to turn away from this conversation. I'm sure we're going to have to follow up with another one. But I do want to get to the issue of tethered cord, because a lot of people asked it, even in the chat just now I saw it come up.
Why is it-- and I guess this kind of also dovetails into another question that we have-- why is it that tethered cord is so often missed? How is it appropriately tested for? Is it a matter of radiology? Do we have to educate the neuroradiology community in some way? Or is there just not enough known about how it presents? Is there any way you can speak to that? And, I guess, how it's treated? Because, at the end of the day, the detethering would be done by a surgeon.
[Dr. Greenfield] Yeah, this has become one of my favorite areas of research. Again, I know it sounds like we're researching everything, but we actually are going to have a clinical trial opening up for occult tethered cord very soon. Because I think it's, again, just like the neuropsych part of Chiari, occult tethered cord is this whole mysterious realm that so many doctors, radiologists, neurologists, either don't understand or just don't believe in.
Unfortunately, the word "occult" pinned onto this disorder has created some of that stigma, I think. I personally think "occult" sounds like witchcraft and attaching witchcraft to a medical diagnosis is a bad combination for malpractice rates. I think there have been practitioners who have pushed the envelope and have done so in a responsible way, such that we learned a lot of important information but I think traditional neurosurgery has been very cautious about adopting it and moving forward too quickly. And I think that the radiologists, and the neurologists are gonna lag behind us.
I think some of the controversy and some of the difficulty just comes from the terminology. And I think if we could explain it better, and describe it better, it'd be much easier. The way that I try to distinguish between tethered cord radiologically and tethered cord syndrome, I think, makes all the difference. If you ask someone if they have a tethered cord, what everyone's gonna think you mean by that, if you're a neurologist, a neurosurgeon or a neuroradiologist, is: do you have signs of a fat-infiltrated filum terminale--do you have what's called "fatty filum"?
Other types of tethered cord, from lipomeningocele, to diastematomyelia-- they can all cause tethering and they all do-- but those are really easy to see.
The less obvious radiologically, the more difficult it becomes to make that diagnosis. And so, if you have a normal "appearing" MRI scan-- with "appearing" in italics, or bold, then it's gonna be twice as hard for you to get this diagnosis.
So, what you have to pivot to, is ask the question... Not "do I have tethered cord?" The question is "do I have tethered cord syndrome?" Tethered cord syndrome is really what makes it much more understandable and palatable for other doctors because what you're then talking about is a constellation of symptoms and signs that can't be otherwise explained by seven different body groups being involved.
The way I think about it is to sort of divide it into orthopedic issues: things like scoliosis, club foot, leg length discrepancies, hip dysplasias. Those are orthopedic issues that may be related to problems with the lower end, the "distal" part, of the spinal cord.
Then there are the neurologic issues. It could be numbness, tingling, it could be weakness I consider pain to be a neurologic issue Low back pain and leg pain in the absence of any other explanation.
Urologic symptoms are right at the center of tethered cord syndrome. So, if you've got a "neurogenic bladder", or a bladder that is not receiving the proper inputs, that's not contracting properly... This is a diagnosis you can get from a urologist very clearly. That is really central to the tethered cord syndrome diagnosis.
Other radiographic findings: do you have a syrinx? Or a terminal ventricle at the bottom of your spinal cord? Do you have any elements of your spinal canal that didn't close properly-- known as "dysraphism".
Do you have skin abnormalities like hemangiomas, or little tufts of hair or little dimples that might be clues? I think putting all those together can create enough of an argument that there is some dysfunction embryologically that relates to the symptoms that the child or adult is now experiencing as a constellation of signs and symptoms. Not a radiographic diagnosis, but a medical diagnosis: tethered cord syndrome.
In those patients, I feel much more comfortable, once they've reached the threshold-- and we can talk about what that may or may not be, I think that's debatable-- then the decision as to whether or not you want to release the filum terminale, even if you can't see anything on the MRI scan, is where the neurosurgical decision- making comes into play.
I think that's a really tricky part of this field. Whether or not it's related to Chiari, I think is something people are curious about. Whether or not tethered cord release can improve Chiari symptoms-- definitely anecdotally people talk about that. Radiographically, you don't see the brain spring back up magically. That doesn't happen. It's just connected in too many different places with nerves and blood vessels-- but you can get symptomatic relief.
It is an important cause of syringomyelia, particularly in the lower thoracic and lumbar areas. So, if you have a syrinx that's really low down in your spinal cord, not up in the cervical area but way low down, that makes me think of tethered cord, as well.
I think it's not a single answer, but rather, a little bit of a medical game of-- you remember that TV show "House". You're putting together all these pieces of information and you're trying to come up with a diagnosis. That's a little bit what it's like.
I just saw a boy today in the office who I'd been suspicious of tethered cord for over a year and we finally got urodynamics done that showed neurogenic bladder and it was kind of like an "a-ha" moment. I think this is it, I think we have it... Normal MRI scan, lots of unexplained symptoms, and this was sort of the piece that we were missing. It took a while to convince the family to get the urologic studies done, but once we did, we were able to move forward.
No one's asking easy questions! These are all really complicated. I hope I'm not going off tangent too much but I think that it does really highlight the complexity of this field and why it's important to think about this broadly and really focus your diagnostic maneuvers based on what you're seeing and not just sort of scattershot patients do the same type of testing across the board.
[voices overlap]
I'm not sure I answered...
[Kaitlyn] I think you got to it. None of the questions are gonna get easier, if that makes you feel terrible, I'm sorry!
So, I guess the next question-- we're gonna kinda stay on the imaging issues here. Firstly, how common is Chiari 0? And I think that should just be a standalone question as far as knowing if it's common, whether or not that's something that needs to be surgically treated? What would you say?
[Dr. Greenfield] So... I don't want to get in trouble here, but I'm not a huge fan of that term... I'm a big believer that you can have Chiari symptoms and you can have syrinx in the absence of herniation, so I don't want to misrepresent how I feel about it....
I think it's come to mean the wrong thing and people have begun using it in the wrong way. You know, Chiari 0 was initially described in a really small sample of patients. It was just an observation by a neurosurgeon that a bunch of patients who didn't meet the criteria for Chiari, had syrinx and they seemed to get better if you did Chiari surgery.
It doesn't really necessarily answer the question as to whether or not it's a specific or separate diagnosis. I think we've all become a lot more comfortable with the idea that you don't need to have 5 mm of herniation to have Chiari symptoms or to have a blockage of CSF to get a syrinx. And so, I think "Chiari 0" really just means "Chiari without a ton of herniation"... and I think that will encompass most of it.
I'm gonna show one other thing here if I can... Let's see...
[silence]
Let me go to my... [clears throat] I'm still sharing, right?
[Kaitlyn] Yes.
[mumbling]
So, this is a talk that I gave just recently at a neurosurgical meeting about something called Chiari 0.5 I've given this talk before to the CSF group and-- basically what it is: in patients who don't have a ton of herniation down the canal, it doesn't mean that you don't have a blockage of flow.
Because I think people often will focus so intently on that one, mid-sagittal view of the MRI scan that everyone thinks of with Chiari. They make the measurement, they see how low the tonsils are... But this is a really important view that I think anyone who's interested in Chiari should really look at this for a second and focus, because this is a cross-section through the brainstem.
And so, the 3-dimensional nature of the brainstem gets lost in those mid-sagittal, or sideways views sometimes. There's CSF that's flowing all around the outside of the brainstem, not just down the back. And so, when your tonsils, represented by these red half-moons here, wrap around and compress the sides of the brainstem, they can also block flow and actually compress a lot of these cranial nerves that are leaving out here.
That can cause problems with swallowing, with breathing, sleep apnea, nausea, vomiting, things like that... So here's just a picture of what this might look like. In a patient who otherwise-- this is a normal MRI for comparison-- who would might otherwise not have a ton of herniation down the brainstem down the foramen magnum into the spinal canal, this is a cerebellum that is wrapping around the side. Here's the brainstem, that little circle right here.. and here's the cerebellum wrapping around the side here.
This is a little girl who actually had a G-tube and could not feed because of severe dysphagia and aspiration. Was decompressed and told that they no longer had any compression, and sure enough on the mid-sagittal view, they looked like they were decompressed, but when you looked at the cross-sectional view, there's no way that the nerves leaving out the side of the brainstem here are not being completely compressed by the cerebellum here.
So, a very focal operation to decompress that... which was highly effective. They came back three months after surgery and she didn't have the G-tube anymore and had gained 20 lbs. It was pretty remarkable.
Not every case works out that well, but I include this because this is such a poignant example of how sometimes one type of imaging can miss it. So, to get back to the Chiari 0 I think there are a number of things that an cause syrinx in the setting of not a lot of herniation. One is this Chiari 0.5, where the tonsils are wrapped around the side. The other is something that's been talked a lot about in recent years and that can be a really simple obstruction of CSF flow at the "obex"-- the obex is a little opening at the bottom of the 4th ventricle-- let me see if I have a picture here...
Hm..
So, right at the very bottom of the 4th ventricle-- you can't really see it here-- there is a little opening. And that's the opening where the "central canal", which is the little tube that runs the entire length of the spinal cord and turns into the syrinx If you get a little, focal blockage of the obex, from a web of arachnoid or tissue or scarring, or a little blood, or any number of things-- an old infection-- then you can get really significant syrinx and, obviously, lots of Chiari symptoms in the absence of any type of Chiari herniation whatsoever.
I think that Chiari 0 is a real thing. I think it's been morphed a little bit to represent something that it's not, but if you feel like you've got a syrinx that isn't otherwise explained, or Chiari symptoms that aren't otherwise explained, do a little bit more digging. Look at the imaging on different planes.
Sometimes you need to do intraoperative exploration, and that comes back to the very thing that these authors from the University of Alabama did: they explored these patients and found that they had obstructions. It takes a lot of guts to define a field like they did. But I think it also points to the role that patients have to push for answers if they don't feel like they're getting the answers they want from their local doctors.
[Kaitlyn] That's good advice. I'm gonna shift a little bit to be very specific to your field. How often should patients get MRIs?
So, I know we have a question where a patient experienced that their syrinx got bigger, or it even moved down or up their spine. And there was also a question about whether or not growth in pediatrics more specifically would affect their Chiari or the development or resolution of a syrinx. How often do you recommend your patients get MRIs? A full cord? Or, not?
What would you say, I guess, about following these patients over time, with or without surgery?
[Dr. Greenfield] And then the growth question. The growth question is an interesting one, so remind me if I don't get to that...
The routine for following patients... The way that I tend to do it is that I get an MRI scan 3 months after surgery. And I used to get an MRI scan at 1 year and do that routinely on everybody.
I'm a little bit more relaxed about that one year MRI scan now, particularly in kids where there may be some need for sedation or if difficulty in getting them. I've become a lot more confident in making sure that we understand the symptoms, educate the parents really well, and rely a lot more on the parents and the symptoms than we do the MRI scan. So, in general, 3 months and 1 year and then after that, really symptom-based.
So, if you're well-- and most of you guys know that kids tend to do well, if they're not complex-- they tend to get done at a year and that's it. And if they come back, we get new imaging because they've got new symptoms. We don't do routine imaging after a year if they're doing well.
For patients that we follow... If you've got a Chiari and you have minimal symptoms and we decide that we're not gonna do surgery and we're gonna follow you, I don't do repeat imaging on any type of schedule that is dictated by the calendar. I'll get a full spine, and if there is syrinx, then I will follow that. I will definitely get a repeat scan of the syrinx because whether or not it's correct or not, I think an enlarging syrinx, to me, is one of the few areas that makes me a little uncomfortable about watching too long.
So, I like to know... If they're asymptomatic and they have a syrinx, I like to know if that thing is getting bigger, or not. Because it might push me over the edge a little bit, even if they're asymptomatic. But not always.
For patients who have no syrinx and just a Chiari, I don't get repeat imaging. We decide how we're going to follow them, decide what metrics are important to the family, keep track of headaches, keep track of symptoms, make sure they're hooked up with a neurologist or their pediatrician is educated, and follow them clinically, getting imaging if they need it.
Ophthalmologic exams are something that we can do routinely. Getting other physicians involved, and really getting to the kids to the age where they can begin to self-advocate because I think the repeat imaging is most useful in some of the very populations where you don't want to do it. So, young kids who can't tell you what their symptoms are, can't self-advocate. Or, kids who have a really large syrinx.
In general, I've become more relaxed with imaging over time. But I do think there's a role for surveillance for peace of mind and for management of syrinx. But it's not always necessary.
In terms of the growth, it goes both ways. I think that for any of you guys out there who have really little kids and have seen me, you know that it's a population that is really tricky to manage because the reoperation rate in little babies with Chiari is really high. And that's because their skulls literally grow back because the factors in the dura that actually create bone are still active and creating bone and the skull is changing.
We try to bide time sometimes by doing a minimal decompression and get them to the point where the skull will actually start growing. And we will see kids actually outgrow Chiari symptoms if they've had them when they're infants.
And we know that from the fact that sometimes they get symptoms back again and when they come back to see me at 8 or 10 years old, and I asked them about the first six months of life, I say, "Did you have trouble feeding your baby?" "Did they have trouble sleeping?" It's invariably "yes," and "yes." So, they probably had Chiari and it was really bad when they were infants because it often is really tight, and then as the skull grows and there's more room, it becomes relaxed.
And that's not something I was trained to recognize or knew, but have observed numerous times. Sometimes you can do that. It doesn't mean that they're going to outgrow it forever, but sometimes it means they can go many years and not need surgery and surgery on really young babies is something that we try to avoid. From anesthetic reasons, blood-loss reasons, and because the re-operation rate is higher.
Once the skull is grown, there's not a whole lot that goes on, to be honest with you. People are often shocked to know how little difference there is between the size of a 3-year-old's head and an 8-year-old's head or a 15-year-old's head. The brain really grows rapidly early in life and the skull is big. You may not notice it, but if you sort of look around and see toddlers running around, they look like lollipops: they've got these big heads and little bodies. The difference between a 3-year-old's head and an adult's head is really not that much in terms of frank percentages, so not a lot goes on.
There's not a whole lot of rationale for scanning patients throughout their lives. It's something that I don't really understand that I see a whole lot. The patients who have changes in their tonsillar herniation, you know, patients who say, "I had an MRI ten years ago and now my herniation is 3mm worse."
There are two populations of patients who will make statement like that. One are patients in whom the MRI scans are identical, but radiologists have read them differently, on different slices, different sequences and the difference between a couple of millimeters means absolutely nothing, but it will sometimes look to new patients or uneducated people in this field that things are getting worse and that's not necessarily the case.
The brain actually moves every time the heart beats. If you've seen any surgical videos, you know it can move 3-4mm with every heartbeat. It goes up and down and the blood fills and empties out of the brain. So, depending on when the MRI captured that image, it can actually look different. So, a couple of millimeters is not real.
If you have an MRI scan that shows that you had no herniation, and now you have 18 mm of herniation, that's not that the Chiari grew-- that is not Chiari malformation. That's a CSF leak, until proven otherwise. Or pseudotumor cerebri, or hydrocephalus, or, God-forbid, a brain tumor. That's something that's causing the tonsils to push down or get pulled down. In those patients, again, Chiari malformation surgery is the last thing you want to do. You need to immediately call you neuroradiologist and say, "I need a myelogram. I need to find where this patient is leaking from."
So, if you have a dramatic change in the size of your tonsillar herniation, it is not that your Chiari is growing. I hope I, sort of, answered all parts of that question there.
[Kaitlyn] You did. You actually answered question that I didn't even ask about Chiari's getting worse over time in that way. So, thank you.
[Kaitlyn] There are three questions...
One came up in the chat, and there are two that I really wanted to get to that were asked before. So, we're gonna go over a little bit and I apologize. But, one of them is very pointed.
What's the usual course kids who have Chiari and scoliosis? So, a lot of the times, they don't have typical Chiari symptoms, they just have the scoliosis. What would you do in the case of a pediatric patient with scoliosis and Chiari, if they're trying to avoid surgery, which is usually the goal?
[Dr. Greenfield] I have this ready here.
[laughs]
So, the Park-Reeves Syringomyelia Research Consortium-- this is an amazing group of surgeons around the country that have all agreed to share their data and the topic of syrinx and scoliosis is a really interesting one, and it's a completely causal relationship.
I work across the street from Hospital for Special Surgery that does tons of scoliosis surgery on kids. We know from seeing all these patients that they now scan every child with scoliosis with an MRI scan, and that didn't happen, I think ten years ago even, as recently as that, that was not the case It was only if they had some neurologic symptoms.
It's now become clear that there's a huge link here and the link is probably related to some type of problem with CSF flow. In patients who have-- the triumphant-- Chiari and syrinx with scoliosis, it is very analogous to this backwards rationale that I used before...
The scoliosis is being caused by the syrinx, because the syrinx is putting pressure on those nerves that are innervating the ribcage and the muscles, the para-axial muscles that support the spine.. and if you have an imbalance there, you start to get a curve and scoliosis is a correction of that.
The scoliosis is caused by the syrinx but the syrinx is caused by the Chiari. And so, you've got to go back up to the top. You can't do scoliosis surgery unless you actually fix the primary problem. So, this is a tough pill for a lot of parents to swallow because you have to explain that they need to have Chiari surgery first, but that doesn't mean that it's going to fix everything and it doesn't mean that you're going to avoid scoliosis surgery.
The easiest way to think about this in terms of an easy ratio-- about 1/3 of patients will get better in terms of their scoliosis after the decompression surgery. About a 1/3 will stabilize, and one third will get worse, despite having surgery done on the Chiari and syrinx. A good percentage of patients will still go on to need corrective scoliosis surgery, but the good news is no orthopedic surgeon who knows what they're doing will ever operate and fix a spine until the Chiari and syrinx has been addressed anyway. Either way, you need to have a neurosurgeon and an orthopedic surgeon working closely together to figure out the timing of those two interventions.
This paper just came out literally-- earlier this spring, I think, from this consortium, looking at the factors associated with the syrinx and how that impacts the scoliosis. It's clear that there are factors that we can now predict a little bit more because of the great collaboration between all these surgeons that the size of the syrinx, the age of the patient-- these things do have an important role in determining whether or not they're going to need to have surgery.
Generally, young kids, big syrinx-- those are the patients who tend to do worse, as you might imagine. So, nothing earth-shattering, but at least scientifically proven that the link is there and it's real. Hard to predict, but certainly something that has some science behind it.
[Kaitlyn] That's great. The question that came up in the chat: are TIA strokes something that might be caused by Chiari or some sort of brainstem, or brain compression? And would decompressive surgery help stop something like that? Or even seizures-- that was another question that had come up.
Would a Chiari decompression help to correct those issues?
[Dr. Greenfield] What-- the first one was… what? Stroke, you said?
[Kaitlyn] Sorry-- TIA. So, mini-stroke.
[Dr. Greenfield] Okay.
Yeah, those are two really interesting questions that are honestly linked together. I would say that for the general consumption-- the vast majority of patients-- I would say no.
Are there examples where I think I can link the two together? Absolutely.
I have anecdotal evidence of patients who have had compression of different parts of the vasculature in the posterior fossa. I published a paper 5 or 6 years ago about a woman in whom we actually opened up, did the decompression and found that one of the arteries was aberrantly placed, and the bone had been pressing that artery for, probably years or decades and it actually caused an area of "ischemia", meaning an area of the brain that never got any blood flow. So, there was evidence of a stroke directly related to it.
I think in most cases, that's not what we find. Those are really severe, unique cases and in patients where they're having TIA symptoms, meaning they're getting lightheaded, or blackouts, or faint, dizziness type of things-- and I think that's probably where this question has its origins-- that's probably more related to dysautonomia, blood pressure, dysregulation.
So, having low blood pressure, having tachycardic syndrome... these are much more common and, I think, probably underreported in the Chiari population. I see them all the time. Clearly, they're really rampant in patients who have EDS and craniocervical instability, but I think even in patients who don't have EDS, I've seen evidence of significant hemodynamic issues. So it may be a component there.
And that's an easy thing to sort out-- well, not easy, but doable. You can get a holter monitor, you can get a Fitbit or a watch that has a heart rate monitor where you can actually monitor your symptoms. Your symptoms now are quite accessible with smart devices, so it might be something that you can either do on your own, or with the help of a cardiologist to get to the bottom of that.
The seizure question-- I'm personally fascinated by. No one else in the world seems to be, so I'm curious who asked that question. Maybe we could have another conversation.
I'm pretty sure that there are-- just like there are connections in the cerebellum that are causing cognitive dysfunction in Chiari patients, I'm similarly intrigued by the idea that compression in the posterior fossa may also cause epileptigenic activity.
We don't ever see it because when we do EEGs and we measure for seizures, we put electrode ledes on the top of the head, no one ever actually monitors the cerebellum.
I've been curious and interested potentially in looking at monitoring some patients, looking at their electrical activity on their cerebellum during surgery, or before and after surgery and seeing that. I haven't pursued that, but I think it's likely that you'll hear some stuff about that in the next few years.
If you ask a neurologist, or an epilepsy doctor if Chiari can cause seizures, they'll send you out of the room and slam the door in your face. So, be careful!
[laughter]
[Kaitlyn] So there's just two more questions, I promise. I hope they're not too complicated.
One is really specific to recovering from surgery. So, there was a patient who was 6-months out after decompression, she-- he or she, actually, I'm not sure-- was still feeling weak and had a lot of pain in their neck and upper back. So, they were curious is this part of the healing process? Is this normal? Or, should something be done 6-months out when you're still having these issues? Or even 12?
[Dr. Greenfield] Yeah, that's a little specific in terms of their own recovery, but I think that in general, there's a pretty huge spectrum of recovery scales.
I think as I became more accustomed to this variability, I became a little less rigid in my definition of what a normal recovery would be. You know, people ask what a recovery would be-- I usually still say 4-6 weeks, but I think that's until you can get back to some semblance of functioning.
In terms of pain and recovery and full range of motion, or not needing to be on any pain medications or muscle relaxants-- you know, some patients take up to a year to recover. So, I think there's a huge variability there. I think the underlying question there may have been: is there something else going on? And I think that's always a question.
This question of failed Chiari surgery is something that still intrigues me and bothers me about my own patients. I see a ton of patients with failed Chiari from elsewhere, but I definitely have my own patients that have failed. And knowing when do you think you've given it enough time and it's not going to get better? When do you think it's time to go back in and re-explore? When is it time to consider etiology that you might have missed like craniocervical instability? Or did you miss a CSF leak? Or did you miss a pseudotumor? Or did those things come up after surgery?
I can't say in general that there's a rule of thumb on that, except that some patients take a really long time and if you're not getting better, or if you're getting worse (in particular)
then don't be shy about going back and saying, "look, I don't think everything is right here.. is there anything that we can do to explore this?" It may not be an easy road at that point, but certainly try to find someone that will work with you to try and sort through those problems.
It's definitely one of the trickiest things that we face in this field. I feel for you right now, but give it some more time, if you can. But if not, go back to your surgeon and start going down that list of conditions that we've talked about.
[Kaitlyn] A lot of this is back-and-forth with your clinician. And I mean, I wish there was an easier way to do it, but there's really not.
So, the last question really has to do with the state of Chiari research as it is now.
I know a lot of the questions that we had from patients that you answered, you showed papers that had been published not a couple of weeks ago. What's going on in the Chiari, syringomyelia, related disorders research world? And is there anything that, I mean, obviously I know that there's stuff that we're doing to try to make it move a little faster, but how do you see this advancing over the next 5 or even 10 years?
[Dr. Greenfield] Well, I think that paper I have up here speaks for itself: you have surgeons from every single institution around the country, almost represented here. So, the fact that everyone is working together and are putting aside their, you know, individual aspirations and goals and desires to work as a team and collaborate.
It's pretty obvious just looking at that list of luminaries. That's great to see, and I think that's really going to push the field forward because I think people recognize that publishing your own 15 cases or 20 cases no longer cuts it for research in Chiari, which it used to 20 years ago. I think people are also becoming a lot more aware of these co-morbid conditions that all the patients seem to know about but none of the doctors seem to know about
And I think that's eventually going to trickle down. What I've personally tried to do to move the needle, at least in my own neighborhood, is to work with the gatekeepers.
I gave grand rounds to the entire department of neurology and gave --and look that's kind of going into the lion's den. A lot of neurologists don't think that surgery is the right thing for a lot of patients with Chiari and so, I kind of stood up there and took arrows for a while, but I said these are the things that have changed in the last 20 years, this is what we know, these are our outcomes. You need to diagnose this, you need to refer these patients. Just because you send a patient to a neurosurgeon, doesn't mean they're going to end up with surgery. And I think that was always part of their fear.
I'll just say, what we're doing I think, is working. Getting out to the community, educating patients and educating the gatekeepers-- the neurologists, the pain management doctors-- to know about these conditions and provide the right referrals is ultimately is going to be the goal.
The one area where I feel like we're a little bit stuck is on radiology. I'm not exactly sure that's going to be as easy to infiltrate. They don't necessarily read our literature. They'll produce reports that don't mention Chiari sometimes and I've seen this so many times from patients that the frustration of finding out 5 years later that their MRI scan done five years prior had a Chiari on it and they were not told because it wasn't on the report.
It's gonna require a little bit even more level of infiltration because there are so many independent radiologists who are working at radiology centers and freestanding businesses that have MRI machines. And so, I'm not sure I have a great answer for how to do that, except that we've got to keep trying to go out there and educate our colleagues in those fields to move it forward.
But ultimately, I think it's going to be you guys. I think patients are the ones who have moved this forward. Just for, maybe an inspirational close here-- the other part of my life that's not taking care of Chiari patients is taking care of kids with brain tumors and I've been so similarly impressed with how the community of parents who have kids with brain tumors have self-mobilized to say, "You know what? Pharmaceutical companies aren't taking care of us. Researchers aren't taking care of us. We're gonna do it ourselves." And they raised money and started foundations and got research and have made tremendous strides in 20 years. So, sometimes it takes the feeling of not being heard or not being taken as a serious group of patients to mobilize together and create enough of a voice so that the research does get done. This is what the Park-Reeves initiative is, that's a family-run organization that put money behind this. And you guys are giving money to CSF to run these consortiums that are doing the same thing.
I think it's all moving in the right direction and I've never seen better research or more robust rate of publication. So, as long as people are sharing and reading and implementing what we learn, the needle will move forward. If people stay stuck in their ways of doing things and aren't willing to think about occult tethered cord, or think about EDS as a co-morbidity, or look for CSF leaks, then a lot of patients are going to get missed and potentially get hurt by having the wrong surgeries. I think we're heading in the right direction, but we're certainly not there yet and that's why we need these forums.
I appreciate you guys sharing all these great questions and being a part of this. I think I'm happy to continue to be a part of this and to continue to try and provide information when I can, and similarly, try and nudge some of my compatriots, many of whom are on this list here, to do similar forums because I think you might hear variations on a theme, and different approaches and there's no single right answer to many of the questions that you asked today.
Thank you.
[Kaitlyn] Thank you! I know we're definitely going to be reaching out to you-- one of our programs that we're really trying to push and I don't know if it's something we have to do after COVID-19, but we're trying to do some more grand rounds, like you were saying when we started, maybe it's something that we can do virtually where we have someone like you go to another institution, give a grand rounds about why-- even why the radiology is really important like what we talked about with tethered cord where it's not necessarily on the image and sometimes people get better.
I mean, I know we're looking to do all that, so as long as you guys are on-- in our camp, I think we're gonna be good.
[Dr. Greenfield] Awesome. Well, thank you very much everyone! I guess there's no way to say goodbye to 100 people, but thanks for coming.
[overlapping voices]
Thank you so much, Dr. Greenfield.
Thank you.
Thank you, Dr. Greenfield.
It was great, thank you.
Everybody stay safe.
[Dorothy Poppe] And stay tuned, we're going to be doing more of these.
Look forward to it.
[Kaitlyn] We're already planning the next one. Thanks everyone.
Revised: 6/2020